A female’s monthly cycle is regulated by the complex interaction of four hormones including estrogen, progesterone, follicle stimulating hormone (FSH) and luteinizing hormone (LH). FSH and LH are produced by the pituitary gland. They promote ovulation and stimulate the ovaries to produce the female sex hormones, estrogen and progesterone. Estrogen and progesterone stimulate the uterus and breasts to prepare for possible fertilization. The menstrual cycle has three phases: Follicular (before release of the egg), Ovulatory (egg release) and Luteal (after egg release). The regular cycle requires precise levels of the hormones. An imbalance can arise if there is too much or too little of one or more these hormones. Even a minor imbalance or changes in the level of the estrogen and progesterone can cause significant effects with the menstrual cycle and disrupt the normal pattern of the period.
Premenstrual Syndrome
Premenstrual syndrome (PMS) is a combination of physical and emotional symptoms that can occur in between ovulation and menstruation. PMS occurs in the days following ovulation, typically 1 to 2 weeks before the period starts, as estrogen and progesterone levels begin declining rapidly. PMS symptoms typically go away within a few days after menstruation as estrogen and progesterone levels begin rising again.
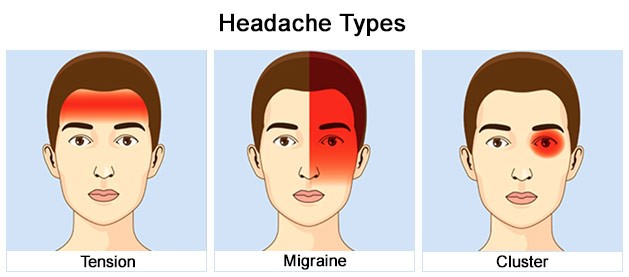
The symptoms of PMS can be categorized into physical and emotional symptoms. Physical symptoms include swollen/tender breasts, constipation/diarrhea, bloating, cramping, headache, and clumsiness. Emotional symptoms include hostile behavior, tiredness, sleep problems, appetite changes, trouble concentrating, anxiety, depression, and mood swings.
PMS is very common with about 80% of women who experience premenstrual symptoms. It has been thought that PMS may be caused by a hormonal imbalance. However, more recent clinical research points out that PMS may also be caused by infection and inflammation of the uterus. The hypothesis that PMS is related to increased inflammation is supported by the evidence that high-sensitivity C-reactive protein (hs-CRP), a biomarker of inflammation, is elevated among PMS patients. Having an hs-CRP level >3 mg/L was significantly associated with physical symptoms such as abdominal cramps/back pain, appetite cravings/weight gain/bloating and breast pain. Infections of the uterus as the cause of PMS was supported by the clinical evidence that both physical and emotional symptoms associated with PMS respond to local anti-inflammatory and antibiotic treatment of the uterus with a stable improvement after the treatment has ended. In summary, the clinical pattern of PMS can be explained as an inflammatory mediated response to uterine infections and traumatic insult.
Premenstrual Dysphoric Disorder
Premenstrual dysphoric disorder (PMDD) is a much more severe form of premenstrual syndrome (PMS). It causes emotional and physical symptoms like PMS, but women with PMDD find their symptoms draining. PMDD symptoms could interfere with patient’s daily life, including work, school, social life, and relationships. The symptoms of PMDD usually show up the week before you start your period and last until a few days after it begins. Symptoms include mood swings, depressions, intense anger and conflict with other people, tension and irritability, Feeling out of control, Cramps and bloating, joint or muscle pain, and/or headaches.
Researchers don’t know the exact cause of PMDD. Most think it may be an abnormal reaction to hormone changes related to the menstrual cycle. Studies have shown a link between PMDD and low levels of serotonin, a chemical in the brain that helps transmit nerve signals. Certain brain cells that use serotonin also control mood, attention, sleep, and pain. Estrogen promotes the positive effects of serotonin. The exaggerated drop in estrogen levels also causes a drop in serotonin levels and effectiveness in women with PMDD which causes the symptoms of depressed mood, food cravings, and impaired cognitive function.
Post Menstrual Syndrome
Post Menstrual syndrome is a combination of physical and emotional symptoms that can occur after a period has ended. The symptoms are quite similar to the symptoms of PMS, but they tend to be more emotional including brain fog, anxiety, moodiness, mood swings, feeling of depression, irritability, anger, and sometimes rage or crying very easily. Compared to PMS, which is popular and occurs in younger women, post menstrual syndrome is less common with about 10% of women and mostly occurs in older women.
The cause of the condition may be the retention of some of the uterine lining from the previous period. The uterine endometrium changes throughout the menstrual cycle. The uterine lining grows during the first part of the cycle in response to the hormone estrogen to prepare the uterus for pregnancy. In the middle of the cycle, an egg is released and levels of progesterone begin to increase. Progesterone prepares the endometrium to receive and nourish a fertilized egg. If pregnancy does not occur, estrogen and progesterone levels decrease. The decrease in progesterone triggers menstruation, or shedding of the lining. The shedding of the lining involves a series of apoptosis, programmed cell death. If such a process does not proceed thoroughly, the lining may not be completely shed. The unshed lining can become necrotic and release toxins into the bloodstream which will irritate the liver causing emotional symptoms.