Allergic diseases affect a large portion of the population and can range from seasonal allergies to asthma. An allergy is an overreaction of our immune system to a particular foreign antigen, also called an allergen. Allergens including plant pollens, foods, chemicals, antibiotics, and mold spores are non‐pathogenic and not themselves harmful, but they can cause an immune overresponse and result in tissue damage.
The immune response is dependent on the body’s two subsets of T-lymphocytes, known as T helper cells, TH1 and TH2. In a normal immune response, TH1 cells release a range of mediators to help the body to defend against invasion from parasites, bacteria, and viruses. In individuals who suffer from allergies, the TH2 cells and their mediators encourage the immune system to recognize allergens as invaders and activate a response against them. In such individual, the antigen is not “learned” by the T cells as tolerable due to their genetics or other factors that have caused Th2 deficiency in antigen recognition.
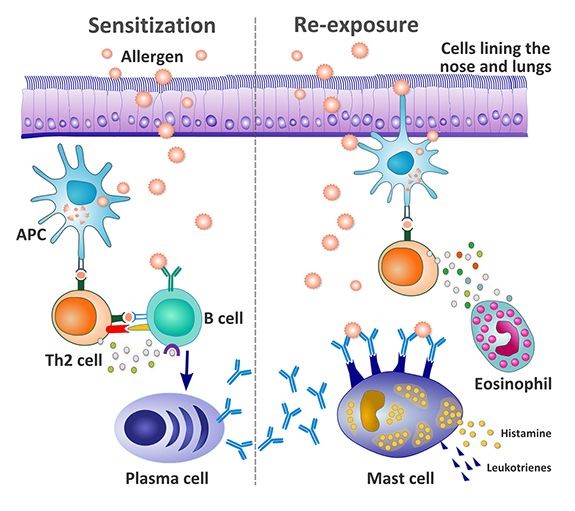 For an allergic reaction to occur, allergen sensitization must first be initiated. In the allergen sensitization process, antigen-presenting cells, such as macrophages and dendritic cells in the mucosal surfaces of the body, detect the allergen. This can occur in many ways, including inhalation into the nose and lungs, through the skin, and through the gastrointestinal tract. In people predisposed to allergies, the antigen-presenting cells come into contact with the allergen which is perceived to be an invader. The allergen is then absorbed, processed and displayed on the surface of the antigen-presenting cell. This process is known as antigen presentation. This cell then presents the processed antigen to the T cells (TH2 cells) and the T cells may recognize them using cell receptors which then stimulates the B-cell to produce IgE antibodies specific to the allergen. These specific antibodies are then released and attach themselves to high-affinity receptors on the surfaces of mast cells in the mucosal surfaces and on basophils in the blood.
For an allergic reaction to occur, allergen sensitization must first be initiated. In the allergen sensitization process, antigen-presenting cells, such as macrophages and dendritic cells in the mucosal surfaces of the body, detect the allergen. This can occur in many ways, including inhalation into the nose and lungs, through the skin, and through the gastrointestinal tract. In people predisposed to allergies, the antigen-presenting cells come into contact with the allergen which is perceived to be an invader. The allergen is then absorbed, processed and displayed on the surface of the antigen-presenting cell. This process is known as antigen presentation. This cell then presents the processed antigen to the T cells (TH2 cells) and the T cells may recognize them using cell receptors which then stimulates the B-cell to produce IgE antibodies specific to the allergen. These specific antibodies are then released and attach themselves to high-affinity receptors on the surfaces of mast cells in the mucosal surfaces and on basophils in the blood.
Following the period of sensitization described above, there is a period of latency and on subsequent re-exposure to the allergen the allergic response is triggered: allergen cross-links with the IgE on the surfaces of the mast cell or basophil, causing the cell to ‘degranulate’ or release inflammatory mediators. These include large amounts of histamine and other mediators, including leukotrienes, prostaglandins, and kinins. These chemicals increase vascular permeability, smooth muscle contraction, secretion of mucus, thinning of the blood causing inflammation and tissue damage. These inflammatory mediators have different actions in terms of symptoms in different organs. In the lungs, this can cause wheezing, shortness of breath, and coughing. In the sinus, this can cause itchy and watery eyes, runny nose, and sneezing. In the blood, it can cause hay fever. The release of heparin from the mast cells can thin the blood and patients may experience bloody nose and/or anus bleeding. Pro-inflammatory cytokines can cause spleen inflammation resulting in an increased blood cell disintegration with the platelets being turned over too quickly. Patients may develop internal bleeding such as stomach bleeding as a result of the decreased platelet count.
Asthma
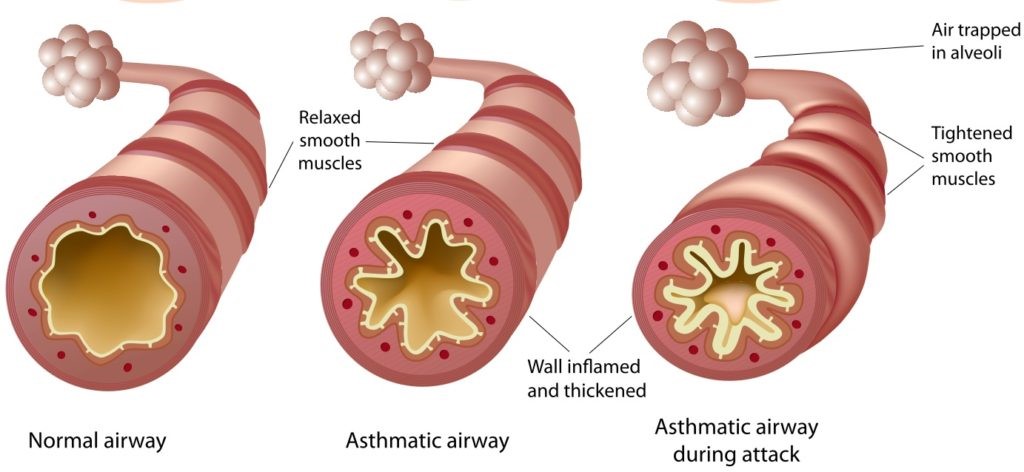
In the lungs, high levels of histamine and other pro-inflammatory mediators caused by the allergic reaction create chronic inflammation and narrowing of the airway which is the pathological event underlying most asthma cases. Symptoms can include, wheezing, coughing, and chest tightness as the airways become restricted and inflamed. The symptoms may flare-up with difficulty breathing during an asthma attack when the smooth muscles of the airways become restricted. Asthma symptoms can occur immediately (early-phase response) or some hours after allergen exposure (late-phase response). Many immune cells and mediators are involved in the asthmatic response and all play a role in the evolution of both the early and late responses. In the early asthmatic response after allergen exposure, inflammatory mediators, including large quantities of histamine, are released from mast cells on the mucosal surfaces. Histamine causes immediate bronchoconstriction and bronchospasm, resulting in narrowing of the bronchioles. Leukotrienes, also released from mast cells, are also potent bronchoconstrictors of airway smooth muscle, amplifying the action of histamine. Leukotrienes also increase microvascular permeability, resulting in edema and narrowing of the airways and stimulation of the secretion of mucus in the lower respiratory tract. Prostaglandins, released by mast cells, are also involved in the early-phase response.
 The late asthmatic response involves the infiltration of the airways with inflammatory cells and mediators, in particular eosinophils, which results in airway narrowing and associated bronchial hyper-responsiveness with bronchial smooth muscle over contraction. Atopic individuals who have the genetic tendency to develop allergic diseases have increased levels of the cytokine inflammatory mediator IL-5 produced by their immune cells such as mast cells and T-lymphocytes. This IL-5 mediator stimulates the production of eosinophils and also attracts them to the site of inflammation. Eosinophils play an important role in the pathophysiology of late response asthma and the associated inflammation and bronchoconstriction. They produce a host of enzymes, proteins, and mediators causing epithelial tissue damage. This damage contributes to chronic changes such as airway remodeling and airway hyper-responsiveness. Symptoms can include shortness of breath as well as an increased chance of lung infections as the lining of the airways can become damaged, making it easier to allow bacteria to harbor. In severe cases, the asthmatic airway can lead to the development of COPD.
The late asthmatic response involves the infiltration of the airways with inflammatory cells and mediators, in particular eosinophils, which results in airway narrowing and associated bronchial hyper-responsiveness with bronchial smooth muscle over contraction. Atopic individuals who have the genetic tendency to develop allergic diseases have increased levels of the cytokine inflammatory mediator IL-5 produced by their immune cells such as mast cells and T-lymphocytes. This IL-5 mediator stimulates the production of eosinophils and also attracts them to the site of inflammation. Eosinophils play an important role in the pathophysiology of late response asthma and the associated inflammation and bronchoconstriction. They produce a host of enzymes, proteins, and mediators causing epithelial tissue damage. This damage contributes to chronic changes such as airway remodeling and airway hyper-responsiveness. Symptoms can include shortness of breath as well as an increased chance of lung infections as the lining of the airways can become damaged, making it easier to allow bacteria to harbor. In severe cases, the asthmatic airway can lead to the development of COPD.
In chronic allergic asthma cases, the individual’s bronchial epithelium is not fully matured and inflammatory cells and eosinophils are accumulated in the bronchial mucosa. This allows allergens to easily trigger allergic reactions with airway inflammation and smooth muscle constriction continuously. The lack of tissue maturation also increases the susceptibility of the bronchial epithelium to allergen-induced injury with an ineffective repair mechanism during chronic allergen exposure.1 It is similar to that observed in chronic wounds and pathological scaring which involves massive apoptosis of inflammatory cells and accumulation of myofibroblasts. The epithelialization remains incomplete and epithelial integrity can’t be restored and the inflammation can’t be resolved.1 This leads to tissue remolding with the extracellular matrix deposition and deformation of the normal tissue causing irreversible airflow obstruction and impaired pulmonary function.
Seasonal Allergies and Allergic Rhinitis
The symptoms of allergies can occur both seasonally and perennially and are caused by a variety of allergens. Offending allergens can often be identified by matching the timing of symptoms experienced by the patient and the prevalence of allergens at particular times of the year. Hay fever is the most commonly experienced seasonal allergy and can occur in spring, summer, and early fall. These allergies are typically brought on by airborne mold spores or pollen from trees, grass, or weeds. Symptoms of hay fever include runny and stuffy nose, itchy and watery eyes, sneezing, itchy throat, and fatigue.
Asthma is usually diagnosed in childhood and in many patients, the symptoms will disappear or are significantly reduced after puberty. After the age of 20, symptoms may begin to reappear. In some cases, asthma is first diagnosed at the age of over 20 years old, e.g. at the age of 50, 60, or even later. This type of asthma is called adult-onset asthma. Unlike children who often experience intermittent asthma symptoms in response to allergy triggers or respiratory infections, adults with newly diagnosed asthma generally have persistent symptoms including wheezing, dry cough, shortness of breath after exertion, and chest tightness. Childhood-onset asthma is usually atopic asthma which is caused by allergies from bronchi tissue immaturity. Although ~30% of adult asthma cases are triggered by exposure to irritants such as cigarette smoke, chemicals, mold, dust, or other substances commonly found in the person’s environment, many adult-onset asthma cases are non-atopic and are not triggered by an allergen involving T cells and IgE. Non-atopic asthma does not involve T cells and IgE and is caused by smooth muscle constriction in both the bronchi and blood vessels that supply blood to the bronchi as well as the resulting airway inflammation. In non-atopic asthma patients, the constriction of the smooth muscle of the blood vessels can cause a reduction in blood flow to the bronchi. Low oxygen supply causes an increased level of free radicals which irritate the bronchi and cause bronchi inflammation. The smooth muscle constriction is induced by internal toxins from infections such as a virus, mycobacteria, other infectious agents, or hormonal fluctuations caused by conditions such as menopause.
Seasonal allergies typically affect the sinus cavities and can also have an early and late phase. In the early-phase reaction, mast cells in the nasal mucosa start degranulation when the allergen is cross-linked with the IgE on the surface of the mast cells on the subsequent re-exposure following the sensitization process. The degranulation involves the release of proinflammatory mediators including histamine which acts upon cells, nerve endings, and the vasculature in the nose. Histamine plays the biggest role in this process, acting upon nerve endings to produce the symptoms of itching and sneezing, and on the small veins and capillaries, causing vascular permeability, which results in nasal blockage, which is one of the primary symptoms of allergic rhinitis.
Inflammatory cells continue to be recruited after the early-phase. These cells and their mediators sensitize the nose to both allergens and non-specific stimuli. This nasal hyperresponsiveness is a characteristic of the late-phase response; sufferers describe allergy-like symptoms on exposure to a range of stimuli, including strong smells such as bleach, hairspray, and tobacco smoke. During this phase ‘priming’ occurs, where nasal cells are ready to respond to stimuli so that often a smaller amount of allergen is enough to provoke allergy symptoms. Similar to the late-phase asthmatic response, eosinophils play an important role in the late-phase sinus response, with enzymes and proteins being release which cause further tissue damage and inflammation.
Eczema
Eczema is a condition in which patches of skin become inflamed, itchy, cracked, and rough. The most common type of eczema is known as atopic dermatitis (AD). Allergens, foods, stress, and hormones have all been linked to factors that can cause eczema. Epidermal barrier defects in the skin are the initial step in the development of AD. AD is often associated with elevated serum level of immunoglobulin E (IgE) and a personal or family history of atopy. It occurs when there is a skin reaction following contact with an allergen that the immune system recognizes as foreign. This triggers the release of a Th2 cascade similar to that seen in allergy sensitization. The cytokines released by the Th2 cascade, like IL-4 and IL-5, lead to elevated IgE, increased inflammation in the skin, and aggravate the skin barrier defect in AD.
Upwards of 80% of individuals who suffer from eczema also develop food allergies. It has been hypothesized that eczema "landscapes" the body for an allergy, in part, by diminishing the barrier function of the skin. As the structure of skin cells collapses, it not only causes the loss of moisture but allows allergens and irritants to infiltrate vulnerable tissues. This, in turn, triggers an immune response in the form of inflammation. It is believed that this hypersensitizes the immune system to the various allergens it encounters on the skin, causing an exaggerated response when those allergens are later eaten or inhaled. Though food allergies don't cause eczema, they can trigger a worsening of existing eczema symptoms. The process by which flares are triggered can vary by the type of food eaten as well as the immunologic response of the individual. Food allergens cause cross-linking of IgE and activation of mast cells and basophils which release histamines and cause allergy symptoms.