Women go through many health conditions that are specific and unique to females. These conditions can range from pregnancy, menopause, to gynecological issues, such as uterine fibroids and endometriosis. There are many gynecological disorders that affect women including menstruation, urinary tract health, and pelvic floor disorders. Pregnancy issues such as miscarriages and disorders relating to infertility can also affect women.
PMS
Premenstrual syndrome (PMS) is a combination of physical and emotional symptoms that can occur in between ovulation and menstruation. PMS occurs in the days following ovulation, typically 1 to 2 weeks before the period starts, as estrogen and progesterone levels begin declining rapidly. PMS symptoms typically go away within a few days after menstruation as estrogen and progesterone levels begin rising again.
The symptoms of PMS can be categorized into physical and emotional symptoms. Physical symptoms include swollen/tender breasts, constipation/diarrhea, bloating, cramping, headache, and clumsiness. Emotional symptoms include hostile behavior, tiredness, sleep problems, appetite changes, trouble concentrating, anxiety, depression, and mood swings.
PMS is very common with about 80% of women who experience premenstrual symptoms. It has been thought that PMS may be caused by a hormonal imbalance. However, more recent clinical research points out that PMS may be caused by infection and inflammation of the uterus. The hypothesis that PMS is related to increased inflammation is supported by the evidence that high-sensitivity C-reactive protein (hs-CRP), a biomarker of inflammation, is elevated among PMS patients. Having an hs-CRP level >3 mg/L was significantly associated with physical symptoms such as abdominal cramps/back pain, appetite cravings/weight gain/bloating and breast pain. Infections of the uterus as the cause of PMS was supported by the clinical evidence that both physical and emotional symptoms associated with PMS respond to local anti-inflammatory and antibiotic treatment of the uterus with a stable improvement after the treatment has ended. In summary, the clinical pattern of PMS can be explained as an inflammatory mediated response to uterine infections and traumatic insult.
Post Menstrual Syndrome
Post Menstrual syndrome is a combination of physical and emotional symptoms that can occur after a period has ended. The symptoms are quite similar to the symptoms of PMS, but they tend to be more emotional including brain fog, anxiety, moodiness, mood swings, feeling of depression, irritability, anger, and sometimes rage or crying very easily. Compared to PMS, which is popular and occurs in younger women, Post Menstrual Syndrome is less common with about 10% of women and mostly occurs in older women.
The cause of the condition may be the retention of some of the uterine lining from the previous period. The uterine endometrium changes throughout the menstrual cycle. The uterine lining grows during the first part of the cycle in response to the hormone estrogen to prepare the uterus for pregnancy. In the middle of the cycle, an egg is released and levels of progesterone begin to increase. Progesterone prepares the endometrium to receive and nourish a fertilized egg. If pregnancy does not occur, estrogen and progesterone levels decrease. The decrease in progesterone triggers menstruation, or shedding of the lining. The shedding of the lining involves a series of apoptosis, programmed cell death. If such a process does not proceed thoroughly, the lining may not be completely shed. The unshed lining can become necrotic and release toxins into the bloodstream which will irritate the liver causing emotional symptoms.
Postpartum Fatigue and Depression
Postpartum Fatigue involves physical and emotional exhaustion following delivery. Women usually become physically and emotionally exhausted in the weeks following delivery due to the intense labor and the demand of taking care of the baby. In some women, the exhaustion does not improve and instead becomes even worse with general health gradually deteriorating. In some case, patients can suffer severe depression. In some patients, they experience similar symptoms after a miscarriage, and/or abortion.
Postpartum fatigue and depression can be caused by small fragments of placental tissue or a blood clot retained inside the uterus after childbirth, miscarriage, and/or abortion. To shed the placental tissue and clotted blood also requires a process of apoptosis. If the uterus can't initiate a complete apoptosis, these tissues or clots can be retained inside the uterus which can become necrotic and release toxins into the bloodstream. These toxins can cause toxicity to liver and other organs resulting in fatigue, depression, and irregularity of menstrual cycles.
Fibroids, Ovarian Cyst, and Breast Cyst
Uterine fibroids are muscular tumors that grow in the wall of the uterus and are usually benign. They can be classified into three different categories depending on where in the uterus they grow. Submucosal fibroids grow inside the uterine cavity, intramural fibroids grow within the wall of the uterus, and subserosal fibroids grow on the outside of the uterus. In some cases, fibroids, called pedunculated fibroids, can grow on stalks that grow out from the surface of the uterus or into the cavity of the uterus. Fibroids can grow singularly or some cases multiple can occupy the uterus. The size of the fibroid varies from about the size of an apple seed to as large as a grapefruit. In rare cases, the fibroid can become very large.
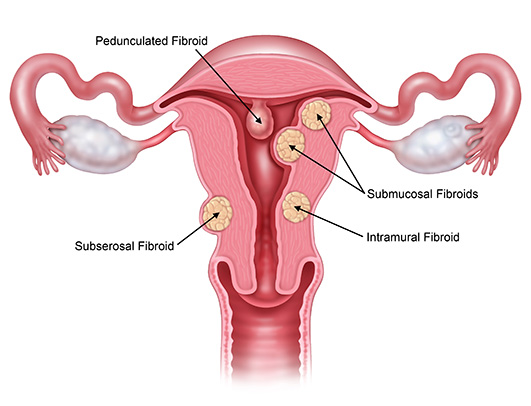
Uterine fibroids are the most common benign tumor in females with an estimated incidence of 20%–40% in women during their reproductive year. Most American women will develop fibroids at some point in their lives. By age 50, 70% of women have had fibroids. In most cases, there are no symptoms associated with fibroids but some patients (~30%) can experience heavy bleeding, feeling of nausea and fullness in the lower abdomen, enlargement of the lower abdomen, frequent urination, pain during intercourse, complications during pregnancy, headaches, back pain, or pelvic cramping.
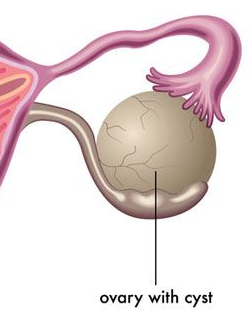
Ovarian cysts are fluid-filled sacs that form in or on the surface of the ovaries. The most common type of ovarian cyst, called a functional cyst, form during the menstrual cycle. The most common types of functional cysts are either follicular cysts or corpus luteum cysts. Follicular cysts form when the follicle that usually releases an egg doesn’t break open causing the follicle to continue growing into a cyst. Corpus luteum cysts form when the follicle sac that usually shrinks into a mass of cells called the corpus luteum doesn’t shrink. Instead, the sac releases itself after the egg is released, and then fluid builds up inside. Other types of ovarian cysts which are less common are endometriomas, dermoids, and cystadenomas.
Most ovarian cysts do not cause symptoms. In some cases, a cyst can cause symptoms of pressure, bloating, swelling, and pain in the lower abdomen. If a cyst ruptures, very severe symptoms occur such as sudden and sharp pain.
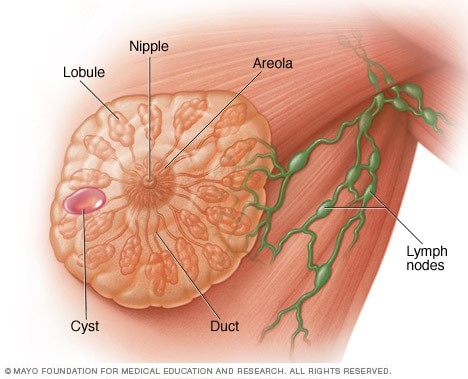
Breast cysts are fluid-filled sacs that form inside the breast and are usually benign. Breast cysts can form singularly or in multiples in one or both breasts. A breasts cyst typically feels like a grape or a water balloon but sometimes they can be firm. They can be classified into two different groups based on their size. Microcysts are often too small to feel and are typically found during imaging. Macrocysts are typically large enough to feel and can cause breast pain and discomfort.
Symptoms of breasts cysts include an easily movable round lump, nipple discharge, breast pain and tenderness, and an increase in breasts cyst size before menstruation. Since the breasts contain lobes of glandular tissue made up of fatty tissue and fibrous connective tissue, breast cysts can form as a result of fluid accumulation inside of the glands of the breast.
The cause of the uterine fibroids, ovarian cysts, and breast cysts have been suggested to be an increased level of estrogen. However, non-surgical treatment that uses estrogen agonists to reduce the circulating estrogen levels has shown only to produce temporary inhibition of the tumor or cyst growth. After the cessation of therapy, rapid regrowth of tumors or cyst usually occurs when normal hormonal fluctuations involved in the menstrual cycle are reestablished. Since the use of estrogen agonists to decrease levels of circulating estrogen has serious side-effects including bone loss and increase in blood lipid levels which increases the risk for early-onset osteoporosis and cardiovascular disease, the long-term use of estrogen agonists is precluded.
Further research has pointed out that reduction of estrogen does not result in programmed cell death, apoptosis of the tumor and cyst, which explain the limited success of the estrogen agonists therapy. The cause of the tumor and cyst development and growth is the reduction or loss of the ability to initiate the activity associated with apoptosis in the female reproductive system.
In fertile women, transient inflammation and uterine lining tissue injury is a physiological and essential process during menstruation, ovulation, and parturition. However, if the damaged cells during the menstruation are not removed completely through apoptosis, the damaged cells can cause the tissue regeneration mechanism to continuously operate, leading to the development and growth of a fibroid. In addition, harmful stimuli, such as irritants or pathogens can trigger dysregulated tissue repair leading to the development and growth of a fibroid.
Mycobacterium infections to the female reproductive tract can cause tissue damage and inflammation. They can also trigger macrophages to engulf the mycobacteria. The immune system reacts to the infected macrophages to form granulomas in which the immune cells and fibroblasts aggregate to form layers surrounding the infected macrophage to seal it inside a barrier from which it cannot escape. The granulomas can lead to the formation of uterine fibroids and ovarian cysts.
Endometriosis
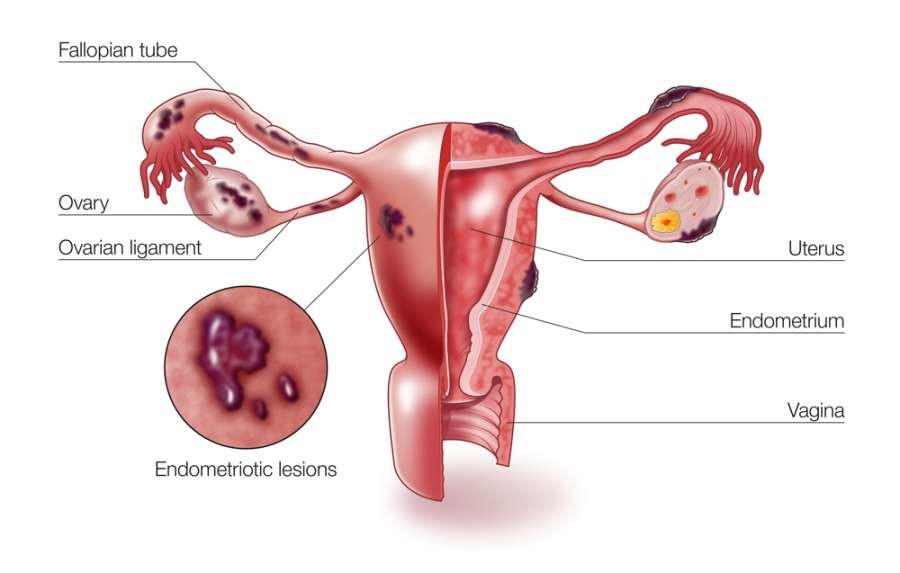
Endometriosis is a painful condition in which the tissue that normally lines the inside of the uterus called the endometrium grows outside of the uterus. The ovaries are a common site for endometriosis to occur. But it can also affect the fallopian tubes and the tissue lining of the pelvis. In rare and severe cases, endometriosis can spread beyond the pelvic organs. With each menstrual cycle, the displaced endometrial tissue continues to act as it normally would. The tissue thickens, breaks down, and bleeds but since there is no way of excreting it from the body, the fluid becomes trapped. This causes surrounding tissue to become irritated and eventually leads to the development of scar tissue and adhesions.
The symptoms associated with endometriosis typically occur during the patient’s menstrual cycle including painful periods, cramping, pain with bowel movements and urination, excessive bleeding, and nausea. Infertility can also occur due to endometriosis based on multiple hypotheses. Cytokines produced by the inflammation can paralyze the effect on the sperm and egg. Endometriosis can also physically distort pelvic anatomy due to the scarring and adhesions which can block the fallopian tubes and ovaries preventing the sperm and egg from coming in contact with each other.
The cause of endometriosis is due to a metabolic deficiency combined with inflammation and/or infection. Although the displaced endometrial tissues act as the normal endometrial tissues, the biochemical and pathological properties are very different between the two types of tissues. Infection and inflammation as a cause of the condition have been supported by research findings. In patients with endometriosis, there are higher numbers of E. coli in menstrual blood, and higher endotoxin levels in the menstrual fluid, as well as, in peritoneal fluid.1 The lower genital tract in humans is regularly exposed to numerous bacteria and the imbalance of microflora may cause an infection, which could then migrate to the upper genital tract and the peritoneal space. The infection and inflammation causes a deficiency in the metabolism resulting in a compromised apoptosis initiation so that cells that are supposed die to keep accumulating.
PCOS
Polycystic ovarian syndrome (PCOS) is a condition in which a higher level of androgen, a male hormone, causes the eggs in the ovaries to not develop or to not be released during ovulation. This can result in enlarged ovaries with numerous small cysts on the outer edges of the ovary. A typical symptom of PCOS is irregular menstruation. PCOS can also cause infertility.

The signs and symptoms of PCOS often develop around the time of a woman’s first period. A diagnosis of PCOS is made when a woman has irregular periods, an excess amount of androgen, and/or polycystic ovaries. The exact cause of PCOS is unknown but factors that may play a role include an excess amount of insulin, low-grade inflammation, heredity, and excess androgen. Excess amounts of insulin in young women can increase androgen production from the ovaries. Low-grade inflammation can also stimulate ovaries to produce more androgen. Complications of PCOS include infertility, gestational diabetes, miscarriage, metabolic syndrome, sleep apnea, abnormal uterine bleeding, and cancer of the uterine lining.
Infertility
Infertility is defined as not being able to get pregnant after one year of trying. Infertility can also be defined as a woman who can get pregnant but is unable to stay pregnant due to multiple miscarriages. Most cases of infertility are caused by problems with ovulation such as when ovulation does not occur or the egg's quality is poor. Polycystic ovarian syndrome (PCOS), hormonal imbalance, inflammation and infection of the uterus can also cause infertility. There are also many other factors that affect a woman’s fertility including age, smoking, excess alcohol use, poor diet, and weight.
A female’s monthly cycle is controlled by the interplay of several female hormones. Four of the main hormones include estrogen, progesterone, follicle stimulating hormone (FSH), and luteinizing hormone (LH). These hormones have to be released in a timely manner. Imbalanced hormones or disruption of the timing of hormonal release will cause an irregular period or loss of period and infertility.
An underdeveloped female reproductive system and insufficient blood supply to the ovaries can cause decreased levels of female hormone production which can cause menstruation issues with symptoms of painful periods, cold feeling, and cycles that are longer than one month with small amounts of blood and clotting. The deficiency in female hormone levels can also cause underdeveloped breasts as well as lower jiao coldness. Patients can develop infertility with symptoms of low sex drive, poor energy level, and fatigue. Patients may experience not only difficulty getting pregnant but also easily have miscarriages.
Menopause
Menopause is the cessation of the menstrual cycle when the ovaries stop producing eggs. It typically occurs after the age of 40 and after 12 months with no menstruation. In the months to years following the cessation of periods, a woman's estrogen level gradually begins to decline. In addition to estrogen, other hormones produced by the ovaries including progesterone, another female hormone, and testosterone, a male androgen hormone also decline during menopause. Such inevitable changes in the hormone levels during menopause can significantly affect a women’s health for years to come. Menopausal women can experience irregular periods, vaginal dryness, fatigue, hot flashes, sweating or night sweats, early awakening or insomnia, thinning of hair, anxiety, dry skin, irritability, moodiness, and a reduced sex drive. These symptoms are caused by the damage brought to the liver and kidney from the physiologic and biochemical changes associated with the decline of estrogen and other hormones levels.
Estrogen exhibits a number of beneficial roles in helping to maintain liver function. These include promoting coagulation, maintain proper fluid balance, and foster increases in high-density lipoproteins and decreases in low-density lipoproteins that lead to favorable lipid profiles. Within the liver, estrogen inhibits proliferation of satellite cells and fibrogenesis which can cause liver fibrosis upon activation and protect the liver from fibrotic tissue formation. Estrogen also protects liver mitochondrial structure and function, inhibits cellular senescence, increases innate immunity, and promotes antioxidants. Menopause represents a state of growing estrogen deficiency. This loss of estrogen in the setting of physiologic aging puts the liver at a great risk of becoming damaged with compromised liver function. It greatly increases the likelihood of liver mitochondrial dysfunction, cellular senescence, declining immune responses to injury, and disarray in the balance between antioxidant formation and oxidative stress. The sum effect of these changes will increase the liver’s susceptibility to the development of significant liver pathology, particularly nonalcoholic fatty liver disease. For patients who already have a liver disease, it will accelerate the progression of fibrosis. Declining liver function can further pose challenges to the kidney causing kidney inflammation and damage as toxins in the blood may not be detoxified properly by the liver.