Lupus is a systemic autoimmune condition in which the immune system attacks the tissues and organs of the body through circulating self-reactive antibodies that deposit in tissues. This can cause inflammation of many body systems including the joints, skin, kidneys, brain, heart, and lungs. Lupus can flare up from mild to serious and most patients have periods when the disease is active, followed by periods when the disease is in remission. There are three main types of lupus which include systemic lupus erythematosus (SLE), discoid lupus (DLE), and drug-induced lupus. SLE can affect any body organ whereas DLE is a milder version that typically only affects the skin. Drug-induced lupus is caused by prescription drugs such as hydralazine, procainamide, and isoniazid.
1 Unlike SLE and DLE which are autoimmune conditions, drug-induced lupus symptoms usually disappear within six months after these medications are stopped.
Symptoms
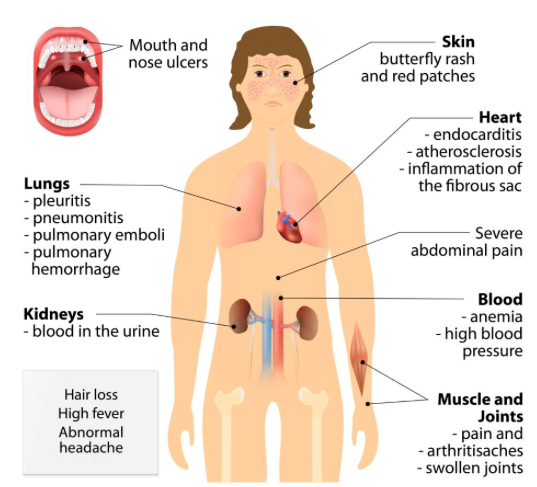
Symptoms of lupus vary and come and go as the disease becomes active. When a patient is having symptoms, it is considered to be a flare-up of the disease. Although symptoms can vary from person to person, the most common symptoms include pain or swelling of the joints, muscle pain, fever, red rashes typically on the face, chest pain, hair loss, sensitivity to the sun, swelling the legs, mouth sores, swollen glands, and fatigue.
Pathogenesis
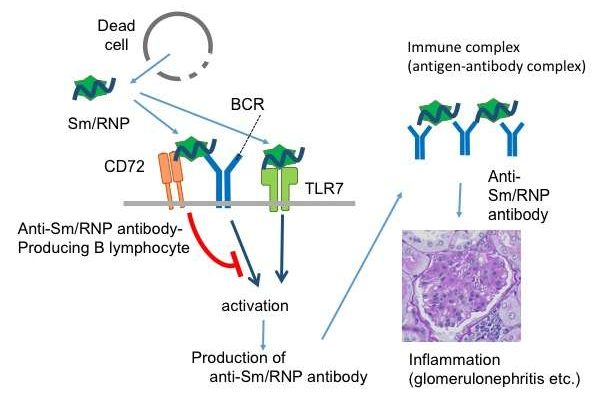
The pathogenesis of SLE is not fully understood and current therapies mainly rely on the use of corticosteroids and cytotoxic anti-proliferative drugs which have limited efficacy and carry significant risks of toxicity. The pathogenesis of SLE is characterized by a systemic loss of self-tolerance with activation of autoreactive T and B cells which lead to the production of pathogenic autoantibodies. This occurs due to immune system’s failure to control autoreactive T cells, B cells, and antigen-presenting cells.2 These autoantibodies bind to nucleic acids and their binding proteins that are released from dead cells to form an antigen-antibody complex. Such complex can trigger local activation of a complement system and cause cell destruction, tissue injury, and organ damage. Hyperactive B cells and loss of B-cell tolerance promote inflammation because pro-inflammatory cytokines not only drive T-cell activation but also leads to the expansion of innate immune cells. Innate immunity also plays a significant role in the development of SLE due to its contribution in both tissue injury via the release of inflammatory cytokines as well as the activation of autoreactive T and B cells.
2 In SLE, organ damage will eventually occur. If left untreated, it leads to serious and even fatal complications such as renal failure.
Although the cause of lupus is not fully understood, researchers have identified that this loss of self-tolerance is a consequence of genetic factors along with environmental triggers. SLE has a strong genetic component and recent genome-wide association studies have discovered several SLE susceptibility genes that are normally responsible for maintaining immune system tolerance.
3 Environmental triggers such as UV radiation, stress, certain medications, and infections can contribute to disease onset.
3 Endogenous retroviruses (ERV) have also been implicated in triggering autoimmunity through structural and functional molecular mimicry with viral proteins.
5
Lupus and Kidney Disease
Lupus nephritis, a type of kidney disease caused by SLE, is one of the more common health problems caused by lupus since the kidney is the primary source of tissue injury in SLE. Autoantibodies initiate and activate tissue-infiltrating macrophages that promote an inflammatory response leading to tissue injury.
4 Symptoms of lupus nephritis include edema and foamy urine and typically begin at the same time or shortly after lupus symptoms appear.
Lupus and the Lymphatic System
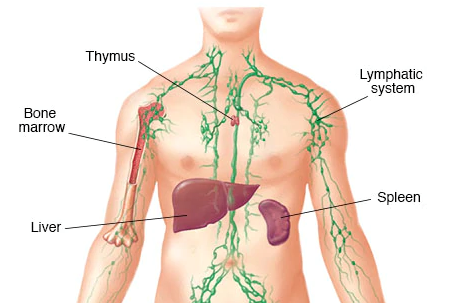
The lymphatic system is a major part of the immune system and it plays a key role in the development of autoimmune conditions. Research results have shown that lymphatic dysfunction and the resulting decreased lymphatic circulation can induce symptoms of autoimmune conditions.
Both B cells and T cells are produced in bone marrow, but B cells mature in the spleen and T cells mature in the thymus. Both the spleen and thymus are key organs of the lymphatic system. Lymphatic dysfunction and poor lymph quality may affect the B cells and T cells maturation and cause their loss of self-tolerance.
Using MRI and ultrasound, researchers further examined the role of the lymphatics in patients with autoimmune conditions such as rheumatoid arthritis and have shown that the lymphatic flow and contraction frequency in patients with autoimmune conditions have been impaired.
6 Lymphatic function is important for self-tolerance. A failure to suppress the immune response to cleared peripheral tissue antigen(s) can result in an autoimmune condition.
7
Lupus and Liver Disease
The liver also plays an important role in immunological activity. The liver has a much more powerful innate immune capability versus the blood due to its enriched macrophage content and natural killer cells. The liver produces suppressor T cells that control T cell activity. Suppressor T cells, are a subpopulation of T cells that modulate the immune system, maintain tolerance to self-antigens, and prevent autoimmune disease.
References:
1. “What Is Drug-Induced Lupus?” Lupus Foundation of America, 2019, www.lupus.org/resources/about-drug-induced-lupus.
2. Choi J, Kim ST, Craft J. The pathogenesis of systemic lupus erythematosus-an update. Curr Opin Immunol. 2012;24(6):651–657. doi:10.1016/j.coi.2012.10.004
3. Gottschalk, et al. “Pathogenic Inflammation and Its Therapeutic Targeting in Systemic Lupus Erythematosus.” Frontiers, Frontiers, 14 Oct. 2015, www.frontiersin.org/articles/10.3389/fimmu.2015.00550/full.
4. Manderson AP, Botto M, Walport MJ. The role of complement in the development of systemic lupus erythematosus. Annu Rev Immunol. 2004;22:431–456.
5. Perl A. Pathogenic mechanisms in systemic lupus erythematosus. Autoimmunity. 2009;43(1):1-6.
6. Schwartz N, Chalasani MLS, Li TM, Feng Z, Shipman WD, Lu TT. Lymphatic Function in Autoimmune Diseases. Front Immunol. 2019;10:519. Published 2019 Mar 20. doi:10.3389/fimmu.2019.00519
7. Mortimer PS, Rockson SG. New developments in clinical aspects of lymphatic disease. Journal of Clinical Investigation. 2014;124(3):915-921. doi:10.1172/jci71608