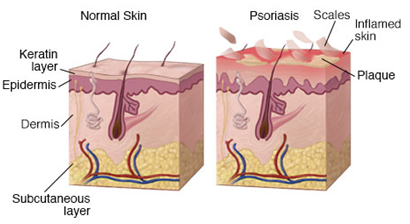
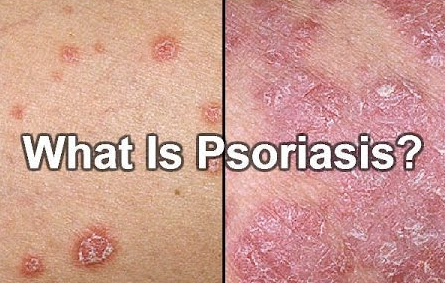
Psoriasis is a chronic autoimmune skin condition in which the life cycle of the skin's cells is greatly accelerated leading to a buildup of dead skin cells on the surface of the epidermis. Typically, skin cells grow deep in the skin and then rise to the surface and eventually fall off. In psoriasis, the extra dead skin cells on the surface form red patches and scales that are often itchy and sometimes painful. Psoriasis scales are often a white-silver color and can crack open and bleed. Scales often develop on the joints like knees and elbows but they can form anywhere such as hands, feet, scalp, face, and neck.
Symptoms:
Along with the thick red patches and silvery scales, symptoms of psoriasis typically include: itching, burning, or soreness, thickened nails, and swollen, painful and stiff joints, as well as general fatigue. There are several types of psoriasis in which most go through cycles in which the condition flares up a for a few weeks or months and then subsides for a period of time.
Causes:
Psoriasis is an autoimmune condition in which white blood cells, called T cells, become over active and attack the skin's cells. This mistaken attack causes the skin cell production process to go into overdrive. The sped-up skin cell production causes new skin cells to develop too quickly and are pushed to the skin's surface where they pile up. The overactive T cells also trigger an increased production of more T cells and neutrophils which travel into the skin and can cause pus in pustular lesions. The dilated blood vessels in the psoriasis-affected area create warmth and redness in the skin lesions. The process becomes an ongoing cycle in which new skin cells move to the surface too quickly, typically in days rather weeks.
The cause of the malfunctioning T cells is still unknown but researchers suspect it may be caused by genetics and environmental factors. Factors such as viral and bacterial infections especially in individuals with HIV or a compromised immune system can increase the risk, stress, obesity, and smoking may also be risk factors.
The liver is an important organ involved in an immune response. Hepatic involvement in adaptive immunity allows clearance of activated T cells and signaling molecules following inflammatory reactions. If the liver is not functioning properly due to any of the above risk factors, the deficient liver can lead to an accumulation of excessive over activate T cells, and can then lead to an autoimmune condition such as psoriasis.
Psoriatic Arthritis (PsA) is an inflammatory form of arthritis also caused by an autoimmune condition. Comparing to Rheumatoid arthritis (RA) which is an autoimmune condition caused by an over production of and anti-citrullinated protein antibodies produced by the B cells, in PsA, the joints are attacked by the body's over active T cells. The joint attack by the T cells lead to symptoms such as pain in the joints, joint stiffness and swelling, physical deformity, and fatigue. Patients with psoriasis have a greater risk of developing psoriatic arthritis (PsA). According to the Arthritis Foundation, 30 percent of individuals with psoriasis develop PsA. Most individuals with PsA have skin symptoms before their joint symptoms appear, but the joint problems can sometimes begin before skin lesions appear. PsA can also occur in people without skin psoriasis, particularly in those who have relatives with psoriasis.
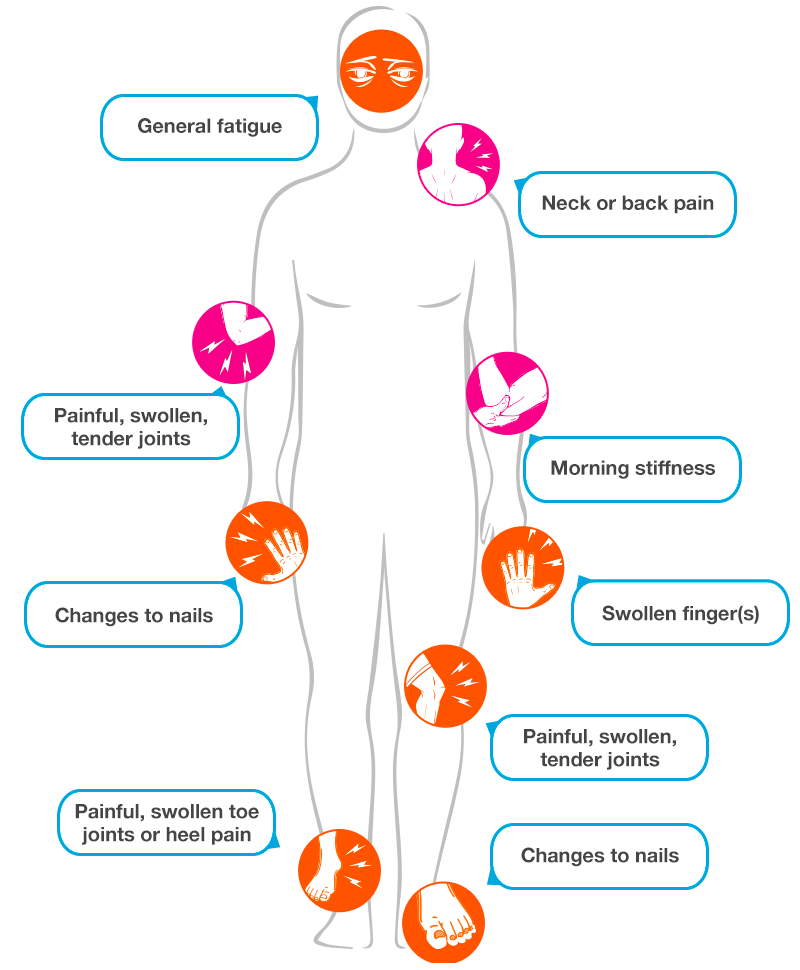
Comparing to RA which is diagnosed using the RF factor, there is no definitive test for PsA and, therefore, PsA is often undiagnosed or misdiagnosed. Patients who present with characteristics of PsA, particularly the pain, swelling, tenderness and stiffness and the inflammation of the tendons and ligaments in the joints, should be further evaluated for the possibility of PsA.
Patients who have liver conditions such a hepatitis, alcoholic liver disease, non- alcoholic fatty liver disease, cirrhosis etc. often develop arthritis with joint pain and inflammation. Since these people do not have psoriasis, their condition is usually not diagnosed as PsA. However, due to the involvement of liver, these cases can be viewed as pseudo PsA. Pseudo PsA is often observed in RA patients, especially in those who have suffered from RA for very long time and their liver is severely damaged due to the long-term use of immunosuppressant drugs.